Lets say your son fails to always give close attention to his school work, overlooks assignment details, and sometimes makes careless mistakes as a result. Additionally, he struggles to stay attentive during lectures and lengthy reading assignments. Your son also does not always listen to you when you are speaking to him, and he doesn’t always follow through on homework and chores. Do you have a child with mental illness, or instead a normal kid who struggles to stay focused when he is bored and/or disinterested with school assignments and household chores? The decision made at this very moment will determine if he is labelled “ADHD” and prescribed psychostimulant drugs indefinitely (from childhood to adulthood), or instead viewed as a normal, healthy kid with a wandering mind and not always interested in boring school subjects and chores at home.

Mental health diagnoses
It is important to remember that unlike physical disease and illness that is measured by means of x-rays, blood work, and MRI images, mental health diagnoses are made by having clients answer a series of questions from a checklist of symptoms, and if a specific threshold is crossed the client receives the mental illness diagnosis. Psychiatric disorders are subjective and far more prone to error compared to physical disease and illness that are objectively measured with little to no doctor/client interference. For example, a physician can read a slide and quickly determine if something potentially dangerous is occurring because he or she can compare a sample against what a normal sample should look like. With mental illness, besides the fact that there are not objective markers to observe, there are additional variables that directly impact whether one is diagnosed with a mental illness:
- The client. Often clients come to a mental health facility wanting to find answers for their distress, and either feign or quickly agree to symptoms when asked. In other cases, since the questions are so ambiguous the client passively agrees without giving much thought to what is being asked. And in still other cases, sometimes the question isn’t fully understood, or the client agrees to questions because he understands that he needs a diagnosis in order to receive a drug prescription. None of these reasons are meant to suggest that every client follows these patterns, but it is important to know that these behaviors do occur, and often far more than we would like.
- The diagnosing clinician. Here again without objective measurement, the clinician is left up to his or her own training and thoroughness when assessing a client for mental illness, and this can be quite the task as you might imagine. The clinician asks questions, often vague questions similar to those discussed at the beginning of this article like “does your son sometimes overlook school assignment details?” In many cases the clinician expects an affirmative answer to these questions (since you are there asking for help to begin with), and before you know it enough boxes are checked and a disorder is assigned. Here again the suggestion is not that mental health clinicians do their jobs poorly, but instead to illustrate the inherent bias and expectations that often accompany subjective evaluations.

The vagueness of the questions
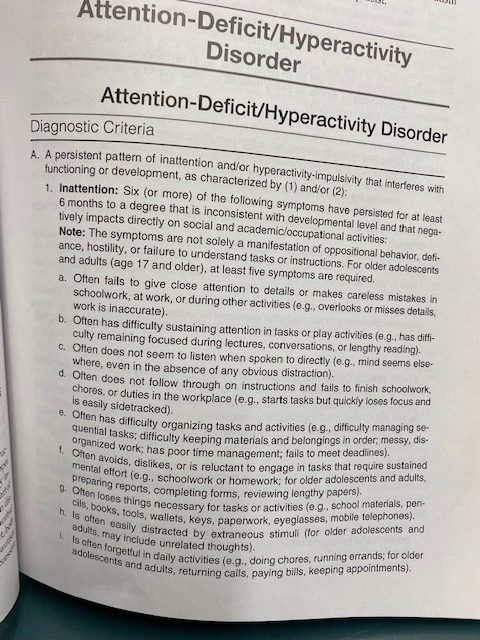
When we use subjective measurements, we are tasked with using our clinical background and knowledge to determine the validity of the answers we receive. Put a simpler way, we have to determine if a client is faking symptoms. Some clients are experiencing so much distress that they will answer that they have nearly every symptom because they want answers, while other clients simply do not fully understand the questions and casually answer yes without thinking much about their responses. Take the following actual ADHD diagnostic question as an example:
“Often fails to give close attention to details or makes careless mistakes in schoolwork…”
- What is “often?” Is “often” 9 out of 10 times, or 5 out of 10? And who keeps a tally to know if something occurs “often?”
- What is “fails?” Does this mean the individual isn’t trying at all, or simply does not fully understand what is being asked?
- What is “to give close attention to details?” What is “close attention,” and how would we ever know the degree of attention a person is directing toward a specific task? And with “details,” what details? Is this referring to the minute specifics, or the entire gestalt of what is happening?
- What are “careless mistakes?” What is careless to one person may have been well thought out, albeit still a mistake, by another. And what if these “careless mistakes” are not psychopathology, but instead evidence of a kid simply bored with school?
From just this simple example (coincidentally, the first symptom category for ADHD) you can see just how many ambiguities there are, and distinctions to make. There is no “secondary manual” clinicians use to specify the terms above, leaving each clinician and client up to their own discretion to figure out exactly what is being asked? And when a client casually shrugs off a “sure” for an answer, rarely do they full understand the magnitude of answering in the affirmative in such a nonchalant way.
Revisit your diagnosis
If you or someone you know has been ascribed the ADHD label, it is strongly recommend you process the following questions:
- Has an authentic diagnosis actually taken place, or has your prescribing physician simply doled out some ADHD drugs to fix your self-reported issues of struggles dealing with focus?
- Have you ever stopped to think that focus and attention are difficult life skills to master, and that it is quite normal for most people to struggle with focus and attention? Over the years pharmaceutical companies have done a terrific marketing job convincing us that only abnormal people struggle with focus and attention, when, in fact, the complete opposite is true.
- If you, or someone you love, has been placed on ADHD drugs do you know the potential side effects of that drug(s)? Furthermore, has the prescribing doctor outlined specific behavioral markers to use to evaluate future progress — and the eventual end of your drug regimen? If no future progress reports are established, how will you ever know if you are improving with your focus and attention?
- Do you know that no drug can direct itself to only adjust the qualities in your life that you don’t like. For example, there is no ADHD drug out there that will only positively impact focus and attention without posing any threat to other more desirable qualities, including spontaneity and creativity.
Ask around and I’m quite sure you will find that many of the people in your life right now have been diagnosed as ADHD. Does it seem odd to you that so many people have ADHD, and that they are told they need a lifelong drug prescription in order to overcome their focus and attention problems? If that seems odd it’s because it is odd, and it’s time to start using our critical thinking to push back on this disturbing and dangerous trend.
Final thoughts
The goal of this column is to raise awareness to the fact that mental illness is diagnosed very differently than other disease and illness, and that because of this quite often both clinicians and clients are left challenged and confused when it comes to making an accurate diagnosis. Compounding matters, how a client is diagnosed will determine dramatically different future paths — if diagnosed with ADHD an uncontrollable biological disorder is assumed, and psychostimulant drugs follow. If, however, the client is not diagnosed as ADHD, he will likely assume his focus and attention challenges are normal, and instead continue to develop healthy life skills in order to achieve greater focus and attention in the future. As you can see, there is quite a bit of weight put into very subjective and often inaccurate diagnostic questions, making it very important for critical thinking when evaluating mental health challenges.
drstankovich.com